
Back in April, midwife sonographer Lis McNulty wrote a blog article about the national fetal anomaly screening programme workshops for screening support sonographers.
I always value getting together as a group of ultrasound practitioners and these workshops provide an opportunity to share learning.
The 2 NHS Fetal Anomaly Screening Programme (FASP) workshops for screening support sonographers (SSSs) held in February this year have helped the national team understand a number of issues facing sonographers.
Strategies to ensure high standards of quality assurance (QA) were high on the agenda. QA is essential in Down’s syndrome, Edwards’ syndrome and Patau’s syndrome screening to drive improvement and give pregnant women confidence in the screening test results they are given.
Areas for improvement
Feedback at the workshop from the Down’s syndrome screening quality assurance support service (DQASS) and sonographers highlighted a number of areas for shared learning and improvement:
1. Individual DQASS nuchal translucency (NT) distribution plots
Some sonographers are not receiving their individual DQASS NT distribution plots. SSSs should share DQASS plots and internal audits with individual sonographers in a timely and constructive manner. Feedback, together with the internal review of images, gives sonographers the chance to improve and enhance their techniques.
2. Interpreting DQASS NT distribution plots
Sonographers should be encouraged to look beyond the flag status, by scrutinising the distribution of the measurements. They should also think about the impact of both the crown rump length (CRL) and NT measurements on the assessment of the screening result, the detection rate, false positive and screen positive rates. For example, they should consider the potential implications of underestimating NT measurements or measuring to the curve.
3. Rounding up or down of measurements
Both CRL and NT measurements should be reported to one decimal point and not rounded up or down to whole numbers.
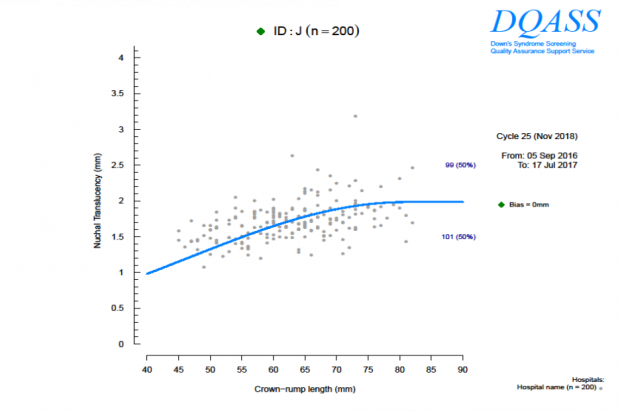
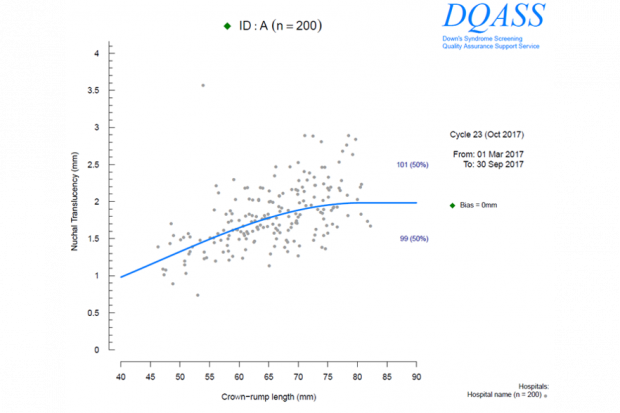
Rounding can be seen in a DQASS individual NT distribution plot, where all measurements stop abruptly at whole numbers, such as 60.0mm or 61.0mm. The actual measurement should be reported, so if the CRL measures 61.3mm, report it as 61.3mm not as 61.0mm (rounded down) or 62.0mm (rounded up).
In the examples below we see a lack of normal distribution in Plot A which indicates that rounding may be happening. Plot B shows a normal disruption that you would expect to see.
4. Hospital summary reports
SSSs should look at the hospital summary reports every cycle. Hospital summary reports provide useful information on overall performance which may highlight issues, such as unsuitable equipment, that affect the whole department.
These reports also provide a plot of the estimated bias relative to Fetal Medicine Foundation (FMF) reference curve (the blue line on the plots above) for each individual sonographer’s data set with 95% confidence intervals. The confidence interval is the range of values within which we are 95% sure the true value of the bias lies.
These intervals depend on the number of scans performed. These plots can help the SSS prioritise support for individual sonographers.
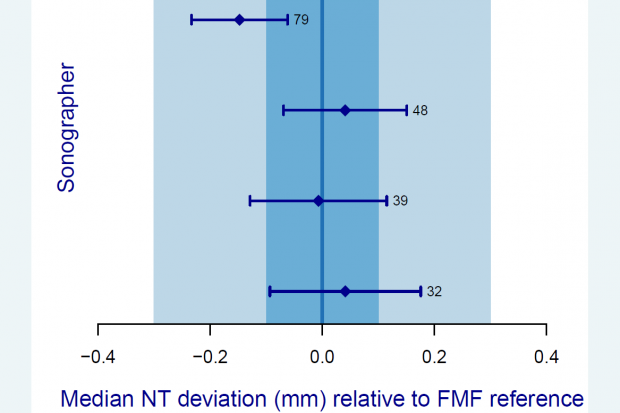
Image reviews
5. Assessing CRL and NT images in conjunction with individual DQASS NT distribution plots
We know it is not always possible to get the perfect images every time. It is therefore important to look at both the CRL and NT images as a complete test. That means looking at the whole picture.
6. Calliper placements
All sonographers strive to obtain the best possible image but calliper placements can let the image down. When faced with factors beyond their control, for example maternal and fetal characteristics, they will use features of the equipment to optimise the image. Once the image is frozen, it is important to take care with calliper placement.
Are the callipers positioned:
- perpendicular to the NT lines?
- on the widest section of the nuchal space?
- on the NT lines?
Is there a nuchal cord?
The nuchal cord appearance can sometimes be very subtle and present as a slight indentation of the nuchal skin line. The correct technique is to take 2 measurements above and below the nuchal cord and take the average instead of a single measurement.
Take home messages
Our main message for SSSs is that you are doing a great job!
Just remember to:
- provide regular feedback to individual sonographers (who should also make sure they receive their individual plots every 6 months)
- encourage and support sonographers to look at both their flag status and their DQASS NT distribution plot
- make sure that CRL and NT measurements are not rounded to whole numbers
Please also remember to interpret all the information received from DQASS to provide a holistic picture of the performance of the department as well as each individual sonographer. This information includes:
- individual NT distribution plots
- hospital summary report including the confidence intervals
- internal review of images
PHE Screening blogs
PHE Screening blogs provide up to date news from all NHS screening programmes. You can register to receive updates direct to your inbox, so there’s no need to keep checking for new blogs.
Recent Comments