We offer screening for sickle cell and thalassaemia (SCT) to all pregnant women. We also offer to screen the baby’s biological father if the mother is found to be a carrier of or have a sickle cell or thalassaemia condition.
SCT screening helps find those at risk and gives parents time to consider the options available to them.
There are several steps in the screening pathway.
- We offer information and screening to the mother.
- Where screening is accepted, we complete the family origin questionnaire and take a blood sample.
- We communicate the result to the mother and, if the mother is found to be a carrier or have a condition, offer screening to the baby’s biological father.
I’d like to focus on the third step. Hopefully the information and advice in this blog article will help healthcare practitioners deal with this complex issue.
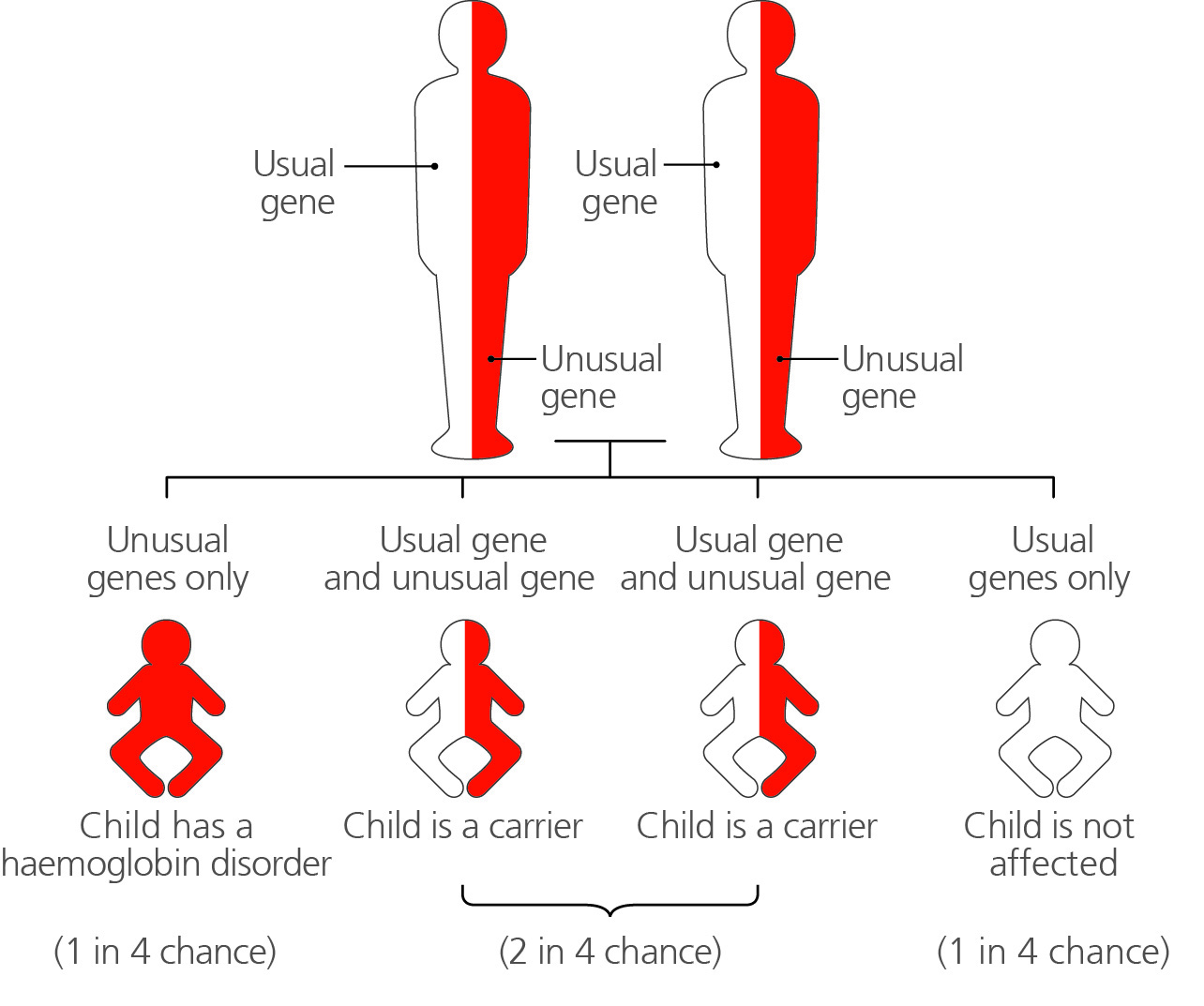
It is really important that mothers understand that the chances of the baby inheriting a sickle or thalassaemia condition relates to the biology (the genes) of the biological mother and father.
Remember that the mother’s ‘partner’ may not be the biological father, so antenatal and newborn screening providers should avoid the word ‘partner’ in this context as it could be misleading.
Also, the father tested in a previous pregnancy may not necessarily be the biological father of the current pregnancy. It is important to sensitively establish if this is the case in order to test the correct father.
In cases where the pregnancy is as a result of sperm donation, the biological father is the sperm donor.
We know that 1 in 6 pregnancies in the UK are unplanned and about 1 in 4 may have some non-paternity issue. We also know there are complexities with testing.
Take home messages
For women who accept the offer of screening, the SCT screening programme recommends screening both mothers and biological fathers (where indicated) in each pregnancy, irrespective of previous results.
In cases where the couple know they have a 1 in 4 chance or higher of having a baby with the condition, blood sampling should happen at the same time as referral for prenatal diagnosis if that is the couple’s choice. The blood test results should then be available when the couple see a clinician. There should be no delays in referrals in these cases.
So there are 4 take home messages.
- Offer and test the biological father.
- Offer and screen in each pregnancy, irrespective of previous results.
- Where ‘at risk couples’ are known there should be no delay in referral to prenatal diagnosis if parents chose this option.
- There should be no delay in referring a woman who chooses prenatal diagnosis if that woman is a carrier, or has the condition, and when the biological father is not available.
PHE Screening blog
PHE Screening BLOG articles provide up to date news from all NHS screening programmes – replacing our previously published newsletters.
You can register to receive updates direct to your inbox, so there’s no need to keep checking for new blog articles.
2 comments
Comment by Jane Raddats posted on
As a sickle cell & thalassaemia specialist midwife I feel that offering a screening test in every pregnancy for a genetic condition that does not change is a waste of NHS resources in a time of increasing pressure on budgets and staff. When the screening programme was set up it was funded for one test per person.
Comment by Nadia Permalloo and Cathy Coppinger posted on
Dear Jane
Thanks for your comment. We review national screening guidance regularly based on feedback from healthcare professionals working in the field, new evidence and any learning from screening safety incidents.
We have recently reviewed our stance on the issue of re-screening in each pregnancy with our professional clinical laboratory advisors. We are currently updating the laboratory handbook to reflect this change.
The decision to test every time was informed by data showing that the majority of laboratories tested every time regardless of previous test results; and informed by screening safety incidents associated with the complexities of the laboratory testing algorithm.
With best wishes